Abstract
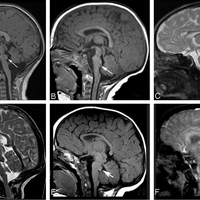
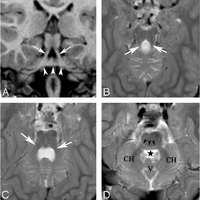
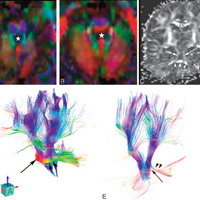
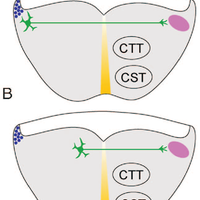
BACKGROUND AND PURPOSE: Malformations of the brain stem are uncommon. We present MR imaging and diffusion tensor imaging (DTI) features of 6 patients with pontine tegmental cap dysplasia, characterized by ventral pontine hypoplasia and a dorsal "bump," and speculate on potential mechanisms by which it forms. MATERIALS AND METHODS: Birth and developmental records of 6 patients were reviewed. We reviewed MR imaging studies of all patients and DTIs of patient 3. Potential developmental causes were evaluated. RESULTS: All patients were born uneventfully after normal pregnancies except patient 6 (in utero growth retardation). They presented with multiple cranial neuropathies and evidence of cerebellar dysfunction. Variable hypotonia and motor dysfunction were present. Imaging revealed ventral pontine hypoplasia and mild cerebellar vermian hypoplasia, in addition to an unusual rounded to beaklike "bump" on the dorsal surface of the pons, extending into the fourth ventricle. Color fractional anisotropy maps showed the bump to consist of a bundle of axons directed horizontally (left-right). The bump appeared, on morphologic images, to be continuous with the middle cerebellar peduncles (MCPs), which were slightly diminished in size compared with those in healthy infants. Analysis of the DTI was, however, inconclusive regarding the connections of these axons. The decussation of the MCPs, transverse pontine fibers, and longitudinal brain stem axonal pathways was also abnormal. CONCLUSIONS: Our data suggest that the dorsal transverse axonal band in these disorders results from abnormal axonal pathfinding, abnormal neuronal migration, or a combination of the 2 processes.
Figures
Register to see more suggestions
Mendeley helps you to discover research relevant for your work.
Cite
CITATION STYLE
Jissendi-Tchofo, P., Doherty, D., McGillivray, G., Hevner, R., Shaw, D., Ishak, G., … Barkovich, A. J. (2009, January). Pontine tegmental cap dysplasia: MR imaging and diffusion tensor imaging features of impaired axonal navigation. American Journal of Neuroradiology. https://doi.org/10.3174/ajnr.A1305
